“I don’t advertise. I don’t do any marketing.”
You can hear the pride when they say it. That slight lift at the end, the way they lean back in the chair. It’s not a confession — it’s a flex. A quiet declaration that their work is so good, their reputation so solid, that customers just… appear.
I hear it most from medical practices. Dentists, physios, specialists who’ve spent 15 years building a patient list through word-of-mouth and sheer competence. They’ve never run a Google ad. They’ve never paid for a lead. And the business works.
Every time I hear it, it breaks my heart a little.
Not because they’re wrong about what they’ve built. They’ve built something real. But because they’re describing the exact dimensions of their cage — and they think they’re describing a castle.
The logic makes sense. That's the problem.
Here’s the thing I want to be honest about: the reasoning behind “I don’t advertise” isn’t stupid. It’s actually quite sound, if you don’t look too hard.
The logic goes like this. A full appointment book means the practice is successful. Referrals mean patients trust the work enough to send their friends. No marketing spend means higher margins. And there’s a deeper belief underneath all of that — a moral one, almost — that good work should speak for itself. That advertising is what you do when your product isn’t good enough to sell on its own.
In medicine especially, there’s a cultural dimension to this. Advertising feels slightly… unseemly. Like something the strip mall chiropractor does, not the serious practitioner. The ones who advertise are the ones who need to. And needing to is the admission of failure.
I get it. I genuinely do. If you told me you’d built a practice to the point where you never had to spend a dollar on marketing, I’d respect the hell out of that. It takes years. It takes consistency. It takes being good at what you do, day after day, until the compound interest of reputation fills your calendar.
That’s not the part I’d challenge.
What "full" actually costs you
The flaw isn’t in the logic. It’s in the definition of one word: full.
When a practice owner says their books are full, they mean they’re busy. Appointments are booked. The days are long. There’s a waitlist, maybe. By every visible measure, the practice is at capacity.
But “full” is doing a lot of heavy lifting in that sentence.
Full of whom? Full at what price? Full on whose terms?
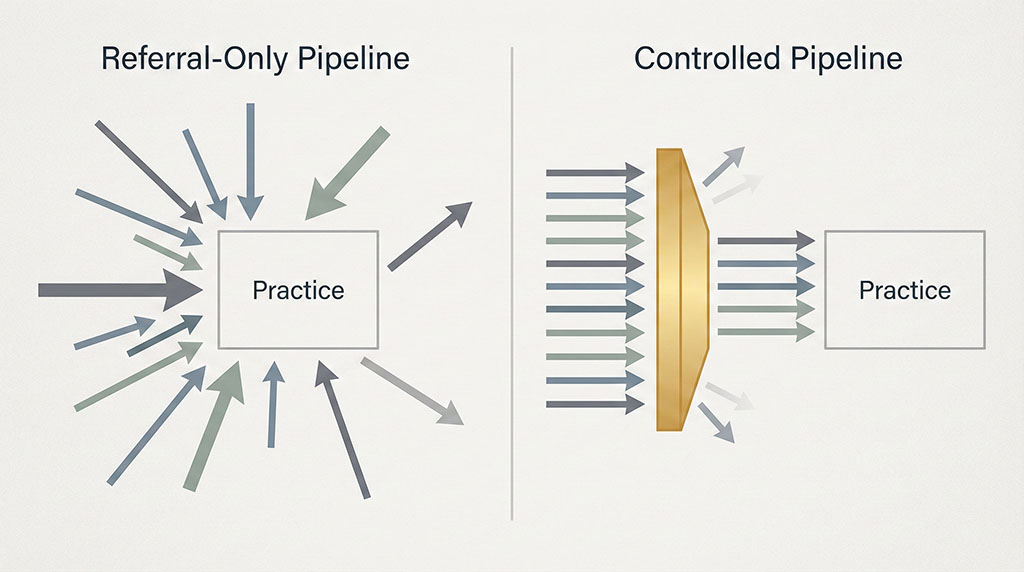
A referral-only practice doesn’t get to choose. Patients arrive through a pipeline you don’t control — someone mentions you at a dinner party, a GP keeps your card on their desk, a former patient tells a colleague. That’s beautiful. It’s also random. You get whoever shows up, at whatever fee they’ll accept, on whatever schedule works for the referral chain.
You can’t select for higher-value cases. You can’t attract the specific conditions you’re most skilled at treating. You can’t test whether a 15% fee increase would even dent demand, because you’ve never had enough inbound to compare.
The practice is full the way a river fills its banks. It looks like capacity. It’s actually just the path of least resistance.
"But it's working."
And maybe it is.
Here’s where I have to be fair, because if I’m not, everything else I say loses credibility. Some practitioners reading this have a practice that runs exactly the way they want it. They earn well. Their patients are great. They leave at 5pm. They don’t want to grow — they want to maintain. And for those people, “I don’t advertise” might be the right answer.
I’m not here to tell someone whose life is genuinely dialled in that they’re doing it wrong.
But that’s not most of the people who say it. Most of the people who say “I don’t advertise” haven’t made a deliberate choice to stay at their current level. They’ve adapted to it. They’ve built their lifestyle, their staffing, their fees, their expectations around a ceiling they’ve never tested. The ceiling feels like stability because they’ve never pushed against it.
And here’s the quiet part nobody says out loud: referral networks aren’t permanent. The GP who sends you 30% of your patients retires. A competitor opens two blocks away with better Google reviews and a booking widget. A hospital changes its referral protocols. One disruption to a pipeline you don’t control, and “I don’t advertise” stops being a badge. It becomes a vulnerability.
The question isn’t whether it’s working now. The question is whether you’ve ever seen what “working” could actually look like.
What the other side looks like: 50 to 4,500
I don’t work with practices that aren’t advertising at all. My clients are typically already spending $5,000 or more a month and want to scale. But the transformation I’ve seen in businesses that go from some marketing to real marketing illustrates the gap I’m talking about.
One client — a roofing company called Roof Buddy — came to me generating about 50 leads per month. Not bad. Busy enough to feel “full.” Sixteen months later, they were generating 4,500 leads per month.
Read that again. Not a 20% bump. Not a doubling. A 90x increase in lead volume in under a year and a half.
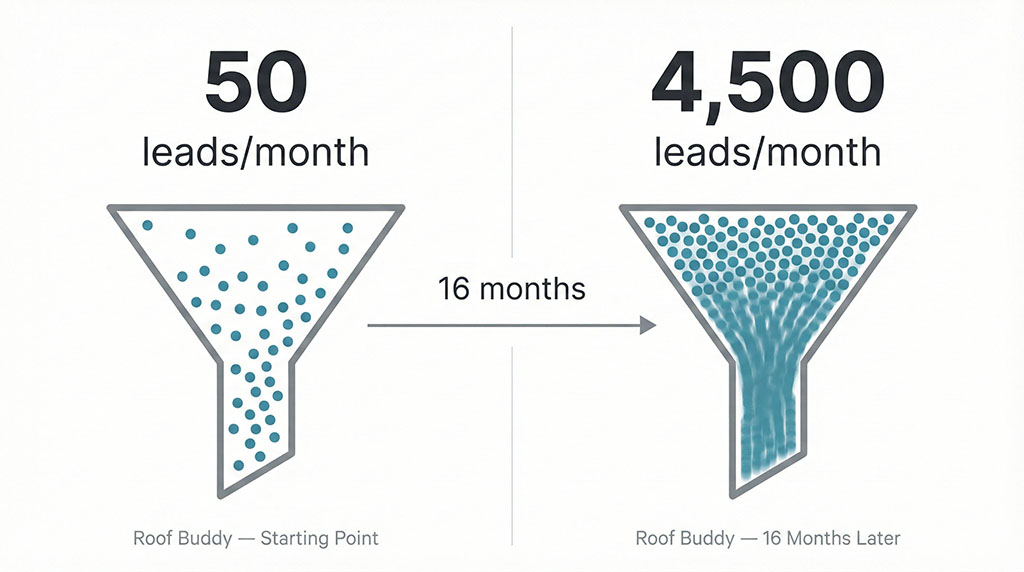
Now — roofing isn’t medicine. The numbers won’t translate directly. But the principle does: the gap between “enough to stay busy” and “enough to choose” is so vast that most business owners can’t even picture it from where they’re standing.
At 50 leads a month, you take what comes. At 4,500, you select the jobs you want, at the price you want, in the locations you want. You hire on your terms. You expand on your timeline. You stop being at the mercy of whoever happens to find you.
That’s what advertising actually buys you. Not patients. Not leads. Options.
Advertising isn't desperation. It's selection.
The deepest misunderstanding buried inside “I don’t advertise” is that marketing is something you do to attract people. It’s not. At a certain level, it’s something you do to filter people.
When you control your inbound, you control everything downstream. You can raise your fees and test whether demand holds. You can market specifically for the high-value cases you enjoy treating. You can build a schedule that works for your life, not just your referral network’s timing. You can stop saying yes to every patient because you’re afraid the pipeline might slow down.
The irony is that the practitioners who say “I don’t advertise” often feel more trapped by their business than the ones who spend aggressively on marketing. Because they can’t adjust. They can’t experiment. They can’t course-correct. The practice runs on reputation and inertia, and the moment either of those wobbles, there’s no backup plan.
Advertising — done properly, as a system rather than a scattered collection of freelancers who don’t talk to each other — gives you the one thing that “I don’t advertise” never can.
Control.
The sentence that should worry you
I’m not going to tell you to go spend $5,000 a month on Google Ads tomorrow. That’s not the point.
The point is this: if you’ve been saying “I don’t advertise” with pride, ask yourself one question. Not whether your practice is full. Not whether your patients are happy. Not whether you’re earning well.
Ask yourself: have I ever seen what’s on the other side?
Because “I don’t advertise” only sounds like confidence when you’ve never tested the alternative. Once you’ve seen what happens when you actually control your pipeline — when you choose your patients instead of waiting for them, when you set your fees based on demand you’ve created rather than demand you’ve inherited — the sentence changes.
“I don’t advertise.”
Same words. But now, if you listen closely, you can hear the ceiling in them.
Your marketing, looked at properly
Thirty minutes on your current setup — what’s working, what’s quietly leaking budget, and what I’d fix first. You’ll leave with a clearer picture whether we work together or not.
Got something specific bugging you? Flag it when you book and I’ll have it looked at before we talk.